- Who We Serve
- What We Do
- About Us
- Insights & Research
- Who We Serve
- What We Do
- About Us
- Insights & Research
America's Healthcare System Is Still Broken
Ignoring U.S. healthcare problems won't make them go away.
By Carl Tannenbaum
Editor’s note: This article is a refreshed version of one we ran a number of years ago. The challenges it highlights for America’s health care system remain unaddressed.
As a young man, my neighbor was the victim of an industrial accident that damaged his knee. The surgery to repair the injury required a long hospital stay and painful rehabilitation. He worked diligently to maintain his mobility, taking up cycling to strengthen his leg.
Over time, though, the discomfort became too great. He opted for a knee replacement; he was up and walking within hours of the operation, and the rehabilitation went much more smoothly than it had 30 years earlier. He got back to cycling quickly; the straightening of his leg proved a convenient excuse to purchase a new $10,000 ride. Bionic joint, bionic bike, he told us.
But while the surgery was a success, there was still some pain to be endured. Within days, bills the length of encyclopedias began arriving at his house, written in language he barely understood. Fortunately, he had good insurance, but he was left to cover considerable copayments.
This story, which is not at all uncommon, illustrates the contradictions in the American health system. For those with access and coverage, treatments have never been better. But the cost of medicine in the United States is unsustainable, and many still don’t have adequate insurance.
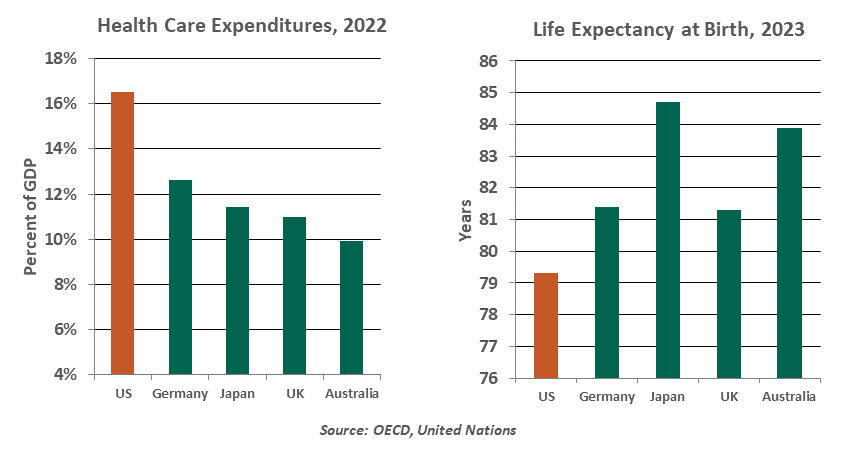
Covering the subject comprehensively would require far more space than we normally allot to our weekly musings. In the main, it seems clear that the system’s costs and benefits are misaligned. The United States spends much more of its national income on health care than other developed countries; the return on this investment, whether measured by life expectancy, infant mortality, cardiovascular fitness or other metrics, is generally worse than what is seen elsewhere.
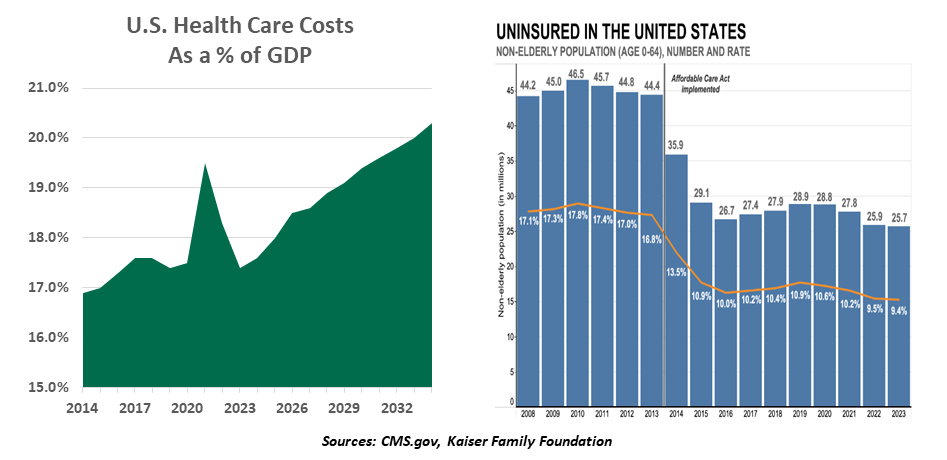
The bill for health care in the United States is projected to exceed 20% of gross domestic product (GDP) within a decade. Demographics are a driver, but studies suggest that the rising costs of individual therapies are also a significant contributor. As well, our citizens (on average) are less healthy and therefore cost more to care for.
Determining the root causes of our healthcare cost affliction is far more complicated than diagnosing patients. Among the leading contributors to cost escalation are:
- Incentives. The profit motive which is ever-present in U.S. care can encourage the overuse of some therapies and the underuse of others. Testing is at times overdone; at other times, insufficient. Preventative care, which can head off costly treatments later on, often requires copayments which some patients cannot afford.
- Administration. About one-quarter of U.S. healthcare costs go to functions that are not directly linked to patient care. The invoicing process is so complicated that it requires a specialized language, mastery of which typically requires several years of education.
- Insufficient Analytics. Healthcare records have become more digitized, but they do not reside on a common platform. Until they are, some of the savings that could be achieved from better diagnostics, consumer choice or more efficient operations will go unrealized.
- Disorganized Demand. Single payer systems are not a panacea, but they do create immense bargaining leverage for health providers. Therapies and drugs often cost substantially more in the United States than they do in other developed countries, mainly for this reason.
- The Tort System. The threat of malpractice claims raises doctors’ insurance rates, which are passed along to patients. And to guard against adverse judgments, physicians may order tests that contribute little to the course of care.
- The Case Management Controversy. Americans spend a significant portion of their lifetime medical expenses during the final weeks and months of their lives. Some therapies have little impact on the length or quality of life at that stage, but families want to do everything for the ones that they love. The proper transition from curative to palliative care is often more humane and less costly.
There is also a challenge with access to the U.S. health care system. According to the Kaiser Foundation, about half of Americans obtain medical insurance through their employers. Another 35% are covered by the two big government plans, Medicare and Medicaid. About 6% purchase insurance directly, primarily through exchanges chartered by the Affordable Care Act (ACA). That leaves about 25 million people without any coverage at all.
These families are vulnerable, both physically and financially, to medical events. When they do fall ill, they often seek treatment at emergency rooms, at considerable expense to the system.
The fiscal legislation passed by the U.S. Congress earlier this month will cut $1 trillion dollars from projected Medicaid funding over the next ten years. It discontinues some elements of the ACA. Some Americans will almost certainly have their insurance coverage curtailed and find themselves at greater risk.
There are those who advocate for a national health system of the kind seen in Canada and many European countries. But a tour through those structures reveals some important imperfections. We might do better to focus our attention closer to home: there is considerable variation in the cost of individual procedures between U.S. states. Studying the root causes of these differences might point the way toward more economical approaches.
The United States isn’t getting any younger, or any healthier. The country’s health care burden will become increasingly acute, using time and money that might better be deployed elsewhere. There are solutions available, but Congress has shown little appetite for reforming the system.
My neighbor fell off his bike recently, leading to yet another expensive encounter at the hospital. Like our healthcare system, he needs to maintain better balance.
Related Articles
Read Past Articles
Meet Our Team
%20scale(1,%20-1)%20rotate(-90.000000)%20translate(-22.445237,%20-21.357547)%20'%20points='21.2928054%2010.2071946%2022.707019%208.79298104%2030.8809213%2016.9668834%2015.4904479%2033.9221138%2014.0095521%2032.5778862%2028.119%2017.034'%3e%3c/polygon%3e%3c/g%3e%3c/svg%3e)
Carl R. Tannenbaum
Chief Economist

Ryan James Boyle
Chief U.S. Economist

Vaibhav Tandon
Chief International Economist
Subscribe to Publications on Economic Trends & Insights
Gain insight into economic developments and our latest forecasts for the United States.
Information is not intended to be and should not be construed as an offer, solicitation or recommendation with respect to any transaction and should not be treated as legal advice, investment advice or tax advice. Under no circumstances should you rely upon this information as a substitute for obtaining specific legal or tax advice from your own professional legal or tax advisors. Information is subject to change based on market or other conditions and is not intended to influence your investment decisions.
© 2025 Northern Trust Corporation. Head Office: 50 South La Salle Street, Chicago, Illinois 60603 U.S.A. Incorporated with limited liability in the U.S. Products and services provided by subsidiaries of Northern Trust Corporation may vary in different markets and are offered in accordance with local regulation. For legal and regulatory information about individual market offices, visit northerntrust.com/terms-and-conditions.