Tough Pill To Swallow
Drug costs are ready targets for policy reform.
By Carl Tannenbaum
When we get together with our neighbors, a round of one-upsmanship often takes place. You got new windows? I redid my kitchen. You got a flashy new bike? I got a flashy new car. You spent a week in Florida? We went to Paris. And so on.
A recent gathering took this exercise in a very different direction. Those assembled started boasting about the sophisticated new drugs they were taking to keep them hale and hearty. The “winner,” if you want to call it that, is taking eight different pills each day to sustain equilibrium.
The folks on my block are not atypical. Consumption of prescription drugs around the world has mushroomed in recent decades, and the cost of those medications has become a significant line item in public and private budgets. For this reason, and others, pharmaceuticals have become a focus area for the U.S. administration.
There is little doubt that breakthroughs in drug therapy have enhanced the length and quality of our lives. The array of GLP-1 drugs has had a dramatic impact on diabetes and obesity. New medications for the treatment of different cancers have been approved in recent years. Genetically-based therapies are being developed to address cystic fibrosis, heart conditions, sickle-cell disease and other maladies.
This is all good news. But these innovations can be very costly. GoodRx estimates that a year’s supply of Ozempic, a leading medication for diabetes, costs up to $15,000 before insurance in the United States. Even with insurance coverage, the costs are substantial for many families. A poll taken by the Kaiser Foundation revealed that 30% of those surveyed had not taken prescribed medication because of cost. This results in chronic ailments getting worse…and more expensive to treat.
There are a series of reasons why Americans pay more for drugs.
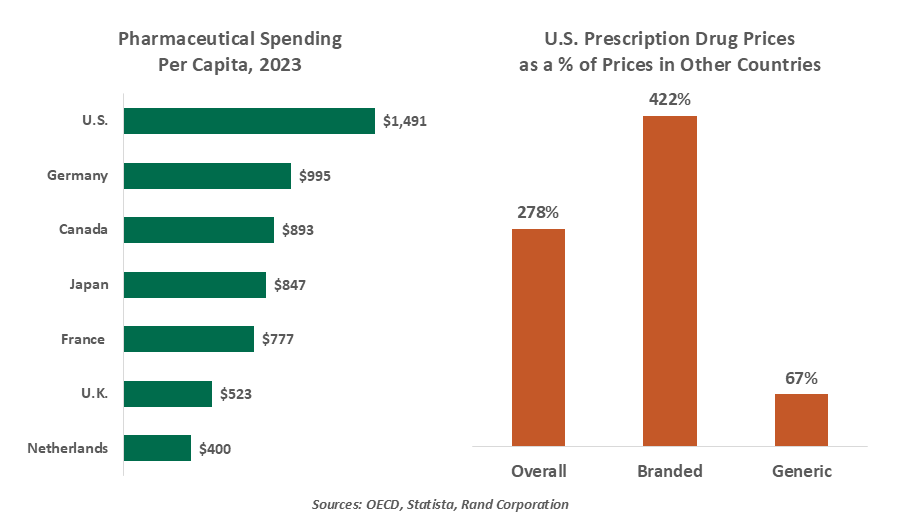
A study from the Peterson Institute found that costs per dosage for U.S. patients are five times more than they are in most other industrial countries. A number of factors contribute to that differential, including:
- Bargaining Power. Many countries negotiate drug prices directly with pharmaceutical firms, often on behalf of a national health insurance system. In the United States, demand is more fragmented: insurance providers negotiate on behalf of the working population, while Medicare does so for retirees. Up until 2022, Medicare could not negotiate with pharmaceutical providers; the Inflation Reduction Act opened this facility, but only for a limited number of medications.
- Insurance Coverage. Americans are much more likely than citizens of other countries to lack health insurance. 27 million people, or 8% of the population, find themselves in this position; recent cuts to funding for Medicaid and the Affordable Care Act may raise these numbers. (This is among the issues at the heart of the current government shutdown.) Those in the U.S. who are covered pay a much higher fraction of drug costs than overseas peers.
- The Availability of Generics. “Name brand” drugs are protected for 20 years after their developer files for a patent. In the U.S., however, pharmaceutical companies often attempt to extend patent protection by making slight alterations to their formulations. A study performed at UCLA found that these tactics cost U.S. patients $52 billion annually. In other countries, generics are much more readily available.
Pharmaceutical providers contend that revenues derived from drug sales are necessary to recoup the investments made to develop them, and to finance future research. An analysis from the Journal of the American Medical Association found that profit margins for large drug companies are almost twice as high as they are for the remainder of the S&P 500.
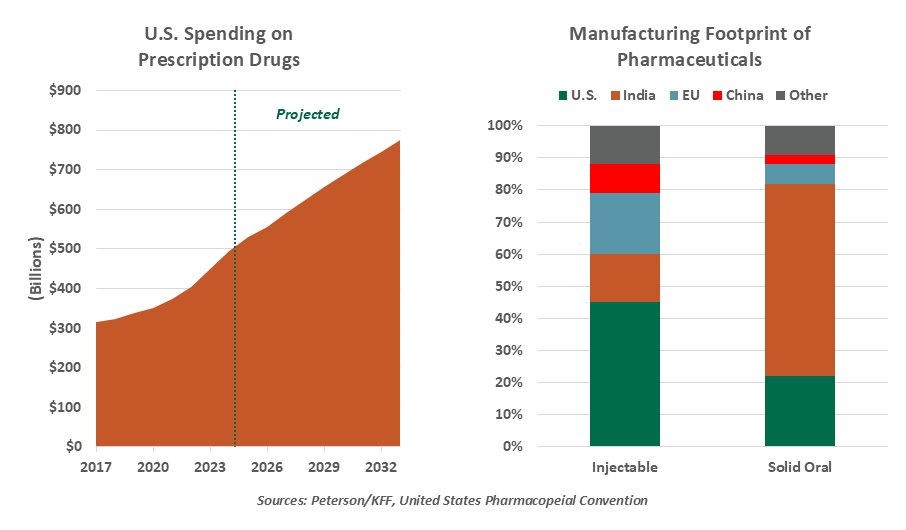
Annual U.S. expenditures for prescription drugs are projected to reach $800 billion by 2033, nearly double the current level. A substantial fraction of this will be paid by the federal government, stressing the budget deficit. It is among the line items that merit the most policy attention.
Over the summer, the Trump Administration turned its attention to this issue. Demands were sent to major pharmaceutical companies, outlining steps to bring U.S. prices more into line with costs in other countries. Tariffs of 15% against providers from the European Union and 100% from elsewhere were threatened if there was failure to comply.
As we have discussed previously, tariff costs are largely borne by consumers. For many medications, drug makers have limited options to re-shore production. Should they be pushed in this direction by U.S. policy, producers like India would be significantly impacted. For these, and other reasons, the administration has proposed off-ramps to avoid the highest threatened tariffs for this sector, like exemptions for firms who plan to increase domestic production.
Despite the headlines, little has been done to change the trajectory of U.S. drug costs.
Pfizer (the largest drug manufacturer in the world by revenue) and AstraZeneca (6th) have reached agreements to lower the prices charged to Medicaid. This is helpful, but limited: the commitments do not cover prices offered to employers, private insurers and other government programs like Medicare. Pfizer also agreed to offer its medications directly to consumers at discounted prices through an exchange named TrumpRx, but those who use insurance to cover their costs will not be able to participate.
So while there is a lot of focus on drug prices, measures taken to date are unlikely to make a meaningful impact on costs paid by the U.S. and its citizens. More fundamental reform would likely take an act of Congress, which would be hotly contested by lobbyists. There is no end in sight for debate on this front.
And there is no end in sight to the status competition on my block. One of my neighbors bragged of obtaining an extra large weekly pill sorter to house her doses; another boasted that his was engraved with his family crest. I think it may be time to move…
Related Articles
Meet Our Team


Subscribe to Publications on Economic Trends & Insights
Gain insight into economic developments and our latest forecasts for the United States.
Information is not intended to be and should not be construed as an offer, solicitation or recommendation with respect to any transaction and should not be treated as legal advice, investment advice or tax advice. Under no circumstances should you rely upon this information as a substitute for obtaining specific legal or tax advice from your own professional legal or tax advisors. Information is subject to change based on market or other conditions and is not intended to influence your investment decisions.
© 2026 Northern Trust Corporation. Head Office: 50 South La Salle Street, Chicago, Illinois 60603 U.S.A. Incorporated with limited liability in the U.S. Products and services provided by subsidiaries of Northern Trust Corporation may vary in different markets and are offered in accordance with local regulation. For legal and regulatory information about individual market offices, visit northerntrust.com/terms-and-conditions.